Erectile function is often discussed as if it operates in a binary way—either working or not working. In reality, it exists on a spectrum that evolves across the lifespan. Subtle changes in erection quality, timing, and responsiveness are common with age, yet these changes are frequently misunderstood. This misunderstanding can lead to unnecessary anxiety or, conversely, delayed recognition of underlying health concerns.
Thank you for reading this post, don't forget to subscribe!Understanding what is physiologically expected—and what may signal a deeper issue—requires looking beyond surface symptoms. It involves examining how blood flow, nerve signaling, hormone balance, and psychological patterns interact over time.
The Physiology Behind Erectile Function Over Time
An erection is not a single event but a coordinated biological process involving vascular, neurological, and endocrine systems. Blood must flow efficiently into penile tissue, nerve signals must trigger and sustain that flow, and hormonal signals—particularly testosterone—must support sexual arousal.
With age, each of these systems undergoes gradual change.
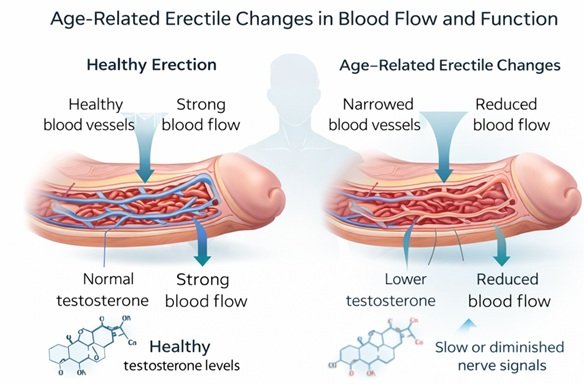
From a vascular perspective, arteries naturally become less elastic. This reduced flexibility can slightly limit how quickly blood fills erectile tissue. Medical research suggests that even minor reductions in vascular efficiency can translate into noticeable differences in erection firmness or speed.
Neurologically, signal transmission may slow. This does not mean dysfunction, but it can alter responsiveness. For example, stimulation may need to be more consistent or prolonged to achieve the same effect experienced earlier in life.
Hormonal changes also play a role. Testosterone levels tend to decline gradually after the age of 30. Studies indicate that while this decline is typically modest, it can influence libido and indirectly affect erectile quality.
These shifts do not occur in isolation—they interact. A small vascular change combined with reduced stimulation and mild hormonal decline can produce a noticeable difference, even if each factor alone would not.
What Is Considered a Normal Age-Related Change?
Normal changes are often subtle and progressive rather than sudden. One of the most common patterns is a longer time required to achieve an erection. This reflects both vascular and neurological adaptation, not necessarily dysfunction.
Another expected shift is variability in firmness. Erections may still be sufficient for sexual activity but feel less rigid compared to earlier years. Healthcare professionals recommend viewing this as part of a continuum rather than a failure of function.
Morning erections may also become less frequent. While often used as a general indicator of physiological health, their decline with age can occur even in otherwise healthy individuals.
Refractory periods—the time required before achieving another erection after orgasm—typically lengthen. This change is well-documented and reflects normal neurochemical recovery processes.
Importantly, these changes tend to develop gradually. A slow transition over years is generally consistent with normal aging patterns.
When Changes May Signal Something More
The distinction between normal aging and potential medical concern often lies in pattern and onset.
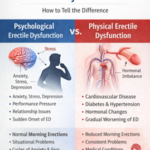
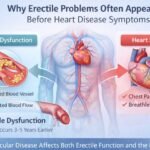
A sudden inability to achieve or maintain an erection, particularly without an obvious psychological trigger, may indicate an underlying issue. Vascular health is a key consideration. Because penile arteries are relatively small, they can show signs of reduced blood flow earlier than larger arteries elsewhere in the body.
Medical research suggests that erectile difficulties can sometimes precede cardiovascular conditions by several years. In this sense, changes in erectile function may act as an early physiological signal rather than an isolated concern.
Consistency is another important factor. Occasional difficulty is common at any age. However, persistent issues across different contexts—partnered and solo, relaxed and stressed—may warrant further evaluation.
Pain, curvature changes, or significant loss of sensation are also not typical age-related developments and may indicate specific medical conditions.
The Role of Psychological Reinforcement
Physiology alone does not explain age-related erectile changes. Psychological patterns often amplify or stabilize these changes.
A common cycle begins with a single episode of difficulty. This may be due to fatigue, stress, or distraction. The experience can create anticipatory anxiety, where attention shifts from arousal to performance monitoring.
This shift alters the body’s stress response. Elevated stress hormones can interfere with the same vascular and neurological processes required for erection. Over time, this creates a feedback loop: concern leads to reduced performance, which reinforces concern.
Studies indicate that this pattern becomes more pronounced with age because individuals are more likely to interpret changes as permanent or irreversible.
Breaking this cycle often involves reframing expectations. Recognizing variability as normal can reduce the psychological pressure that contributes to the problem.
Behavioral Patterns That Influence Erectile Function
Lifestyle factors accumulate over time, and their effects often become more visible with age.
Physical activity plays a significant role in maintaining vascular health. Sedentary behavior can contribute to reduced blood flow efficiency, which directly affects erectile response. Conversely, regular movement supports circulation and endothelial function.
Sleep quality is another critical factor. Poor sleep can disrupt hormone regulation and increase stress levels. Over time, this can influence both libido and erectile consistency.
Substance use, including alcohol and tobacco, also has cumulative effects. While occasional use may not produce immediate changes, long-term patterns can affect vascular integrity and nerve sensitivity.
Dietary habits influence metabolic health, which in turn affects circulation. Conditions such as insulin resistance or elevated cholesterol levels can develop gradually and impact erectile function indirectly.
These behavioral factors do not act independently. They interact with age-related physiological changes, sometimes accelerating or intensifying them.
Understanding the Long-Term Trajectory
Erectile function does not decline in a straight line. Instead, it follows a dynamic trajectory shaped by health status, psychological patterns, and lifestyle choices.
Some individuals experience minimal change well into later decades, while others notice earlier shifts. Studies indicate that variability is the norm rather than the exception.
Importantly, age-related changes do not necessarily progress into severe dysfunction. In many cases, they stabilize. The body adapts, and individuals adjust expectations and behaviors accordingly.
However, ignoring persistent changes can delay the identification of underlying conditions. Healthcare professionals recommend paying attention to trends rather than isolated events.
Distinguishing Between Functional Change and Dysfunction
A useful way to approach this topic is to consider functionality rather than perfection.
Normal aging may involve:
- Slower onset of erection
- Slight reduction in firmness
- Increased need for direct stimulation
- Longer recovery time
Potential dysfunction may involve:
- Persistent inability to achieve or maintain an erection
- Sudden onset without clear cause
- Loss of erections across all contexts
- Associated physical symptoms such as pain or deformity
This distinction emphasizes that not all change is pathological. The key question is whether the changes interfere significantly with sexual activity or quality of life.
How Medical Support Fits Into the Picture
When concerns arise, structured evaluation can help clarify whether changes are within expected ranges or linked to specific conditions.
Healthcare professionals recommend assessing cardiovascular health, hormone levels, and psychological factors as part of a comprehensive approach. This is not about immediate intervention but about understanding contributing variables.
In some cases, discussions may include erectile dysfunction treatment options, which can range from lifestyle adjustments to pharmacological approaches. Studies indicate that medications such as sildenafil-based tablets can support blood flow by enhancing natural physiological mechanisms, though they do not address underlying causes directly.
Equally important is access to medical ED support, which can help contextualize symptoms and reduce unnecessary anxiety.
Why Awareness Matters More Than Perfection
Aging-related changes in erectile function are often framed as problems to be fixed. A more useful perspective is to view them as signals—indicators of how different systems in the body are interacting.
Medical research suggests that paying attention to these signals can support broader health awareness. Erectile function is closely tied to cardiovascular, neurological, and metabolic health, making it a uniquely sensitive marker.
Understanding what is normal reduces unnecessary concern. Recognizing what is not normal supports timely evaluation. Both perspectives contribute to a more informed and balanced approach.
Editorial Policy
This content is written to align with evidence-based health information standards. It is designed to provide educational insight into physiological and psychological aspects of age-related erectile changes. Sources include peer-reviewed research, clinical observations, and established medical understanding. The goal is to present balanced, medically responsible information without promoting specific treatments or outcomes.
Medical Disclaimer
This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Individual health conditions vary, and symptoms related to erectile function should be discussed with a qualified healthcare professional. If you have concerns about persistent or sudden changes, healthcare professionals recommend seeking personalized medical evaluation.